Why aren't we tackling the asymptomatic spread of COVID-19 more aggressively?
By James W. Kim
It is one of the defining features of SARS-CoV-2 that sets it apart from its predecessor SARS-CoV-1: the ability to spread efficiently from individuals who show no symptoms. Yet our testing and containment strategies have been overwhelmingly focused on symptomatic individuals. This is a critical strategic error.
The Asymptomatic Problem
 WHO reported daily COVID-19 cases as of October 31, 2020
WHO reported daily COVID-19 cases as of October 31, 2020
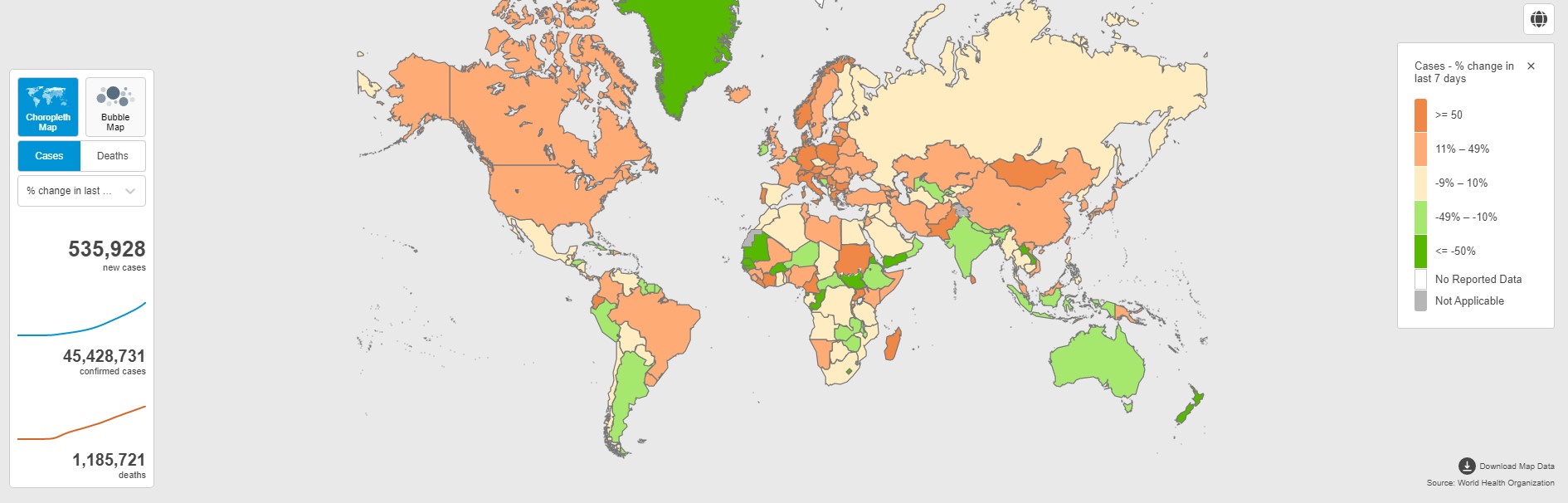 WHO 7-day change in reported COVID-19 cases, October 2020
WHO 7-day change in reported COVID-19 cases, October 2020
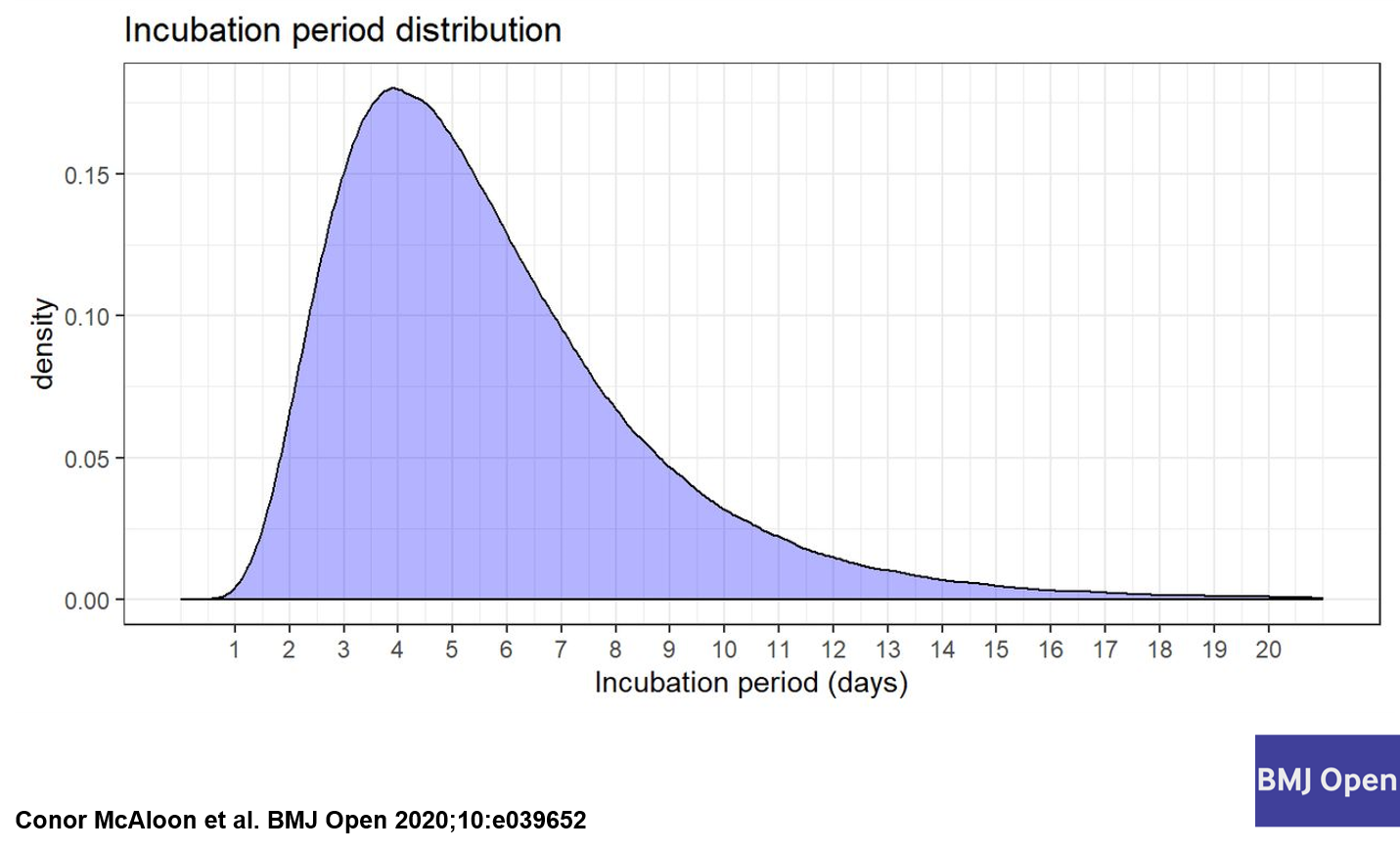
Studies consistently estimate that 20-40% of SARS-CoV-2 infections are entirely asymptomatic. An additional significant proportion are “pre-symptomatic” — infectious before symptoms appear. Together, these groups likely account for the majority of transmission events.
This isn’t new information. We’ve known about asymptomatic transmission since early 2020. Yet most countries’ testing strategies remained focused on symptomatic individuals throughout the pandemic. Testing was — and in many places still is — recommended primarily for those with symptoms or known exposure to a confirmed case.
The logic seems sound on the surface: test the sick, isolate the positive, trace the contacts. But this approach has a fatal flaw — it systematically misses the transmission events driven by people who don’t know they’re infected.
Why We’re Getting It Wrong
Several factors explain this strategic blind spot:
1. Testing capacity limitations. Early in the pandemic, PCR testing capacity was severely constrained. Prioritizing symptomatic individuals was a necessary triage decision when tests were scarce. But as capacity expanded, testing strategies didn’t evolve accordingly.
2. Cost concerns. Mass asymptomatic screening is expensive when relying on PCR tests at $50-150 per test. This is a legitimate concern — but it ignores the potential of cheaper alternatives.
3. Regulatory inertia. Rapid antigen tests — cheaper, faster, and well-suited for mass screening — faced prolonged regulatory review in many countries. By the time they were widely approved, the window for optimal deployment had narrowed.
4. Philosophical resistance. There is a deep-seated resistance in public health circles to “testing the healthy.” This makes sense for expensive, invasive diagnostic procedures, but rapid point-of-care tests change the calculus entirely.
The Case for Mass Asymptomatic Screening
The math is straightforward. If asymptomatic individuals account for a significant share of transmission, and we have the tools to identify them before they transmit, then mass screening is one of the most cost-effective interventions available.
Consider the alternative cost: lockdowns. The economic cost of even a single day of lockdown in a medium-sized city dwarfs the cost of providing rapid tests to the entire population. If frequent asymptomatic screening can prevent even one lockdown, it pays for itself many times over.
The technology exists. Rapid antigen tests can be manufactured at scale for less than $1 per unit. They provide results in 15 minutes. They don’t require laboratory infrastructure. They can be self-administered.
The Right Testing Strategy
An effective testing strategy for a pathogen with significant asymptomatic transmission should include:
1. Frequent, low-cost screening of the general population. Not PCR — rapid antigen tests. Not perfect sensitivity — but good enough to catch most infectious individuals. The goal is not diagnosis; it’s interrupting transmission chains.
2. PCR confirmation for positive rapid tests. Use the expensive, highly sensitive test to confirm, not to screen. This is the most efficient use of laboratory capacity.
3. Targeted high-frequency testing in congregate settings. Schools, workplaces, long-term care facilities, prisons — anywhere people gather regularly should have routine asymptomatic screening programs.
4. Accessible testing infrastructure. Tests should be available at pharmacies, workplaces, and schools — not just at hospitals and testing centers. Every barrier to testing is a barrier to case detection.
Lessons for Future Pandemics
The COVID-19 experience should fundamentally change how we think about infectious disease testing. The traditional paradigm — test the symptomatic, treat the positive — is inadequate for pathogens with significant asymptomatic transmission.
For the diagnostics industry, this represents both an opportunity and a responsibility. The opportunity is in developing next-generation rapid tests that are even cheaper, more accurate, and easier to use. The responsibility is in ensuring these tools are available and accessible in settings where they’re needed most.
For public health authorities, the lesson is clear: testing strategies must be designed for the pathogen, not for the healthcare system’s convenience. If a pathogen spreads asymptomatically, your testing strategy must account for asymptomatic spread.
We have the tools to tackle asymptomatic spread more aggressively. The question is whether we have the will — and whether we’ll apply these lessons before the next pandemic forces us to learn them again.